

You've been told your sperm quality needs improving — whether that's count, motility, morphology, or DNA integrity — and now you want to know the one thing every fertility forum seems to dance around: how long is this actually going to take?
It's a fair question, and the answer starts with one number you need to understand before anything else.
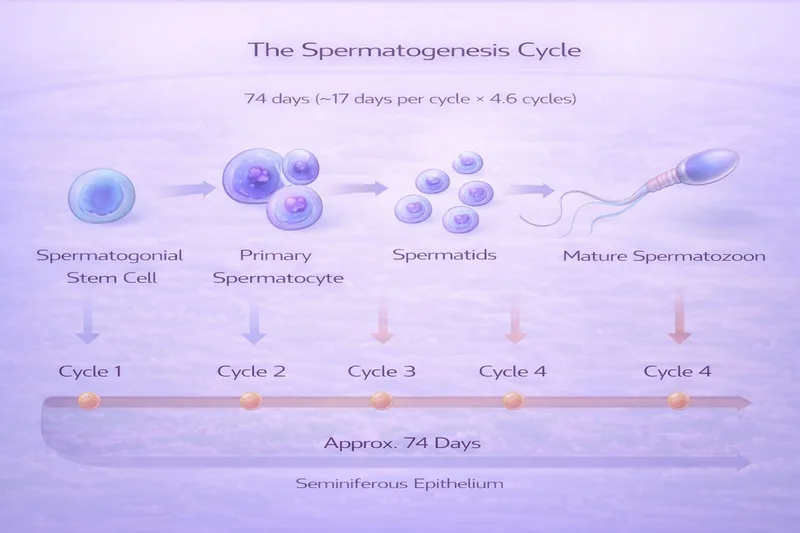
The 74-Day Rule: Why Nothing Works Overnight
Every sperm cell in your ejaculate started its life roughly 74 days earlier as a stem cell deep inside the seminiferous tubules of your testes. This process — called spermatogenesis — involves the stem cell dividing, maturing through meiosis, and transforming into the streamlined, tail-bearing cell we recognise as a spermatozoon (Heller & Clermont, 1964; Amann, 2008).
After those 74 days of development, sperm then spend another 10–14 days maturing in the epididymis, where they gain the ability to swim and fertilise an egg. That means from stem cell to ejaculation-ready sperm, you're looking at roughly 3 months (PMC, 2016).
This is the biological clock behind every timeline in this article. When you make a change today — whether you quit smoking, start a supplement, or have varicocele surgery — you're primarily influencing the sperm that haven't been made yet. The sperm you'll produce over the next few weeks were already well into their development before your intervention began.
This is why the universal minimum for assessing any fertility intervention is 3 months. If someone tells you a supplement "didn't work" after 6 weeks, they haven't given it a fair trial. And some interventions need considerably longer than 3 months.
More recent research using stable isotope labelling has suggested that the total time from spermatogonial commitment to ejaculated sperm may vary between 42–76 days across individual men (Misell et al., 2006; ScienceDirect, 2016). When you add epididymal transit time (10–14 days), the upper end approaches 90 days — which is why many specialists recommend waiting 4–6 months before drawing conclusions.
Quick-Reference Timeline Summary
For those who want the headline figures before the detail:
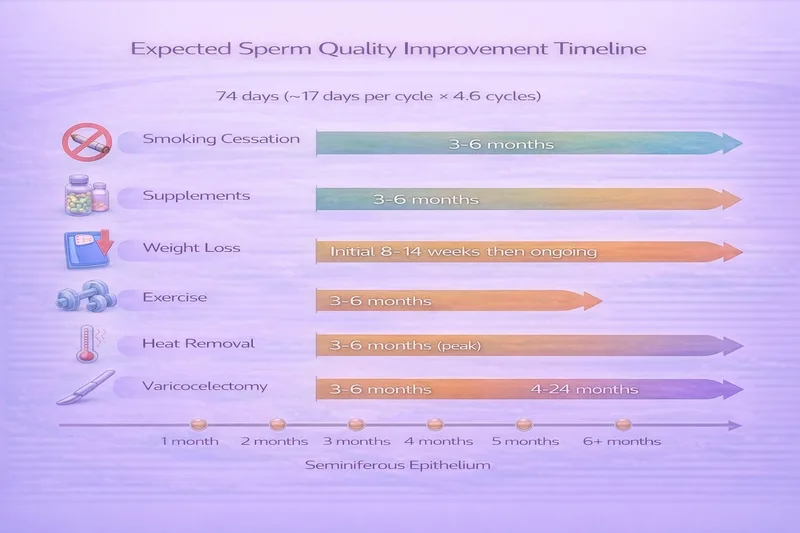
Smoking cessation — First improvements at 3 months, continuing to 6 months
Antioxidant supplements — Allow 3 months minimum, some studies show continued improvement at 6 months
Weight loss (lifestyle) — Hormonal improvements within 8 weeks, sperm parameters 8–14 weeks, maintained with ongoing weight management
Moderate exercise — 3–6 months of consistent moderate-intensity activity
Heat exposure removal — 3–6 months (fully reversible in most cases)
Varicocelectomy — Maximum improvement within 3 months post-surgery
Anabolic steroid/TRT recovery — 4–12 months typical, up to 24+ months in severe cases
Alcohol reduction — 3 months minimum, likely longer for heavy drinkers
Medication changes — Highly variable, depends on the drug (discuss with your doctor)
Now let's look at the evidence behind each of these.
Smoking Cessation: 3–6 Months
Smoking is one of the most evidence-based modifiable risk factors for poor sperm quality. Cigarettes expose the testes to over 4,000 chemicals that cause direct oxidative damage to developing sperm. The good news? The damage is largely reversible once you stop.
A 2022 study followed 48 infertile men who quit smoking (previously 30+ cigarettes per day). At just 3 months post-cessation, they showed significant improvements in semen volume, sperm concentration, and total sperm count (Kulaksiz et al., 2022). However, improvements in motility and morphology didn't reach statistical significance at the 3-month mark.
A more detailed study tracked men at both 3 and 6 months after quitting and found a clear time-dependent pattern — every parameter continued to improve between the two time points (Ragheb et al., 2025):
At 3 months post-cessation: Progressive motility improved from 20.7% to 35.3%, total motility from 41.5% to 60.3%, and abnormal morphology dropped from 69.3% to 50.9%.
At 6 months post-cessation: Progressive motility reached 42.3%, total motility 67.7%, and abnormal morphology continued dropping to 40.8%.
A large cohort study of 1,631 men confirmed these findings, noting that former smokers who had quit more than 6 months previously showed no significant difference in semen quality compared with men who had never smoked (Tang et al., 2019).
A 2025 study using a mouse model also showed that nicotine-induced epigenetic changes (DNA methylation) were partially reversible after cessation lasting at least one spermatogenic cycle (Nature Communications Biology, 2025).
Bottom line: Stop smoking and you should see meaningful improvements in concentration and volume within 3 months, with motility and morphology continuing to improve out to 6 months. Heavier smokers tend to see greater absolute improvements. By 6+ months, your sperm quality profile may be indistinguishable from someone who never smoked.
Antioxidant Supplements: 3–6 Months
Given that oxidative stress is implicated in 30–80% of male infertility cases, antioxidant supplementation is one of the most studied interventions. But which supplements, and how long?
L-Carnitine: 3 months minimum
L-carnitine ranked #1 for improving motility in a network meta-analysis of 23 RCTs, with a SUCRA score of 88.7% and a mean improvement of +12.43% over placebo (Xu et al., 2022). Most RCTs used treatment periods of 3 months at doses of 2g L-carnitine plus 1g L-acetyl carnitine daily. It also ranked first for morphology improvement.
CoQ10: 3–4 months minimum
CoQ10 ranked #1 for improving sperm concentration (SUCRA 79.4%, +5.95 ×10⁶/mL vs placebo) and #2 for motility (+7.33%) in the same meta-analysis. Study durations ranged from 12 to 26 weeks, with most using 200–400mg daily (Xu et al., 2022).
One 16-week RCT using 200mg CoQ10 found increased antioxidant enzyme activity but no significant change in basic semen parameters — suggesting that shorter durations may improve the biochemical environment before visible parameter changes emerge (Nadjarzadeh et al., cited in PMC, 2023).
Combination antioxidants: 3–6 months
A prospective study of 420 men with idiopathic OAT taking a combination antioxidant (SP-Power) measured outcomes at both 3 and 6 months (Kim et al., 2024):
At 3 months: Significant improvements in sperm concentration (8.67 → 12.17 million/mL) and motility.
At 6 months: Further improvements in concentration (→ 19.01 million/mL), with DNA fragmentation index also significantly reduced.
This pattern of continued improvement between 3 and 6 months has been seen across multiple studies, and it makes biological sense — the first 3 months captures one full cycle of spermatogenesis under the influence of the supplement, while by 6 months, two full cycles have been completed.
A comprehensive meta-analysis of 45 RCTs with 4,332 patients found that antioxidant supplementation improved motility, concentration, and morphology, with a spontaneous pregnancy odds ratio of 1.97 compared with placebo (Antioxidants meta-analysis, 2024).
However, it's worth noting that the large FAZST trial found no benefit from high-dose folic acid and zinc supplementation at 6 months — suggesting that the right combination matters, and more isn't necessarily better.
Bottom line: Start your chosen antioxidant protocol and reassess at 3 months with a repeat semen analysis. If you're seeing a positive trend, continue to 6 months. The evidence most strongly supports L-carnitine for motility and CoQ10 for concentration. For a detailed breakdown of supplement evidence, see our Male Fertility Supplements UK guide.
Weight Loss: 8 Weeks to 12+ Months
The relationship between obesity and sperm quality is well established — excess body fat disrupts testosterone production through aromatase conversion, increases scrotal temperature, and drives systemic inflammation. But how quickly does weight loss translate into improved fertility?
Short-term dietary weight loss (8–14 weeks)
The landmark S-LITE trial — a randomised controlled trial — put 56 men with obesity through an 8-week low-calorie diet (800 kcal/day). After just 8 weeks, sperm concentration and total sperm count had significantly improved (Håkonsen et al., 2022). Crucially, men who maintained their weight loss over the following year retained these improvements, while those who regained weight lost the gains.
An earlier pilot study followed 43 severely obese men (BMI 33–61) through a 14-week residential weight loss programme. The group with the largest weight loss showed an increase in total sperm count of 193 million and a 4% improvement in normal morphology (Håkonsen et al., 2011).
DNA fragmentation improvement
Weight loss appears to improve sperm DNA integrity as well as conventional parameters. One study of over 100 men found that mean DNA fragmentation index improved from 20.2% to 17.5% after weight loss, with the degree of improvement correlating with the amount of weight lost (Mir et al., 2018).
A 2024 study comparing low-energy versus basic dietary interventions found that men on the more intensive diet had significantly lower DNA fragmentation at the end of the intervention, with an inverse correlation between weight loss and DFI (Sharma et al., 2024).
A word of caution about bariatric surgery
While lifestyle-based weight loss appears consistently beneficial, bariatric surgery shows more mixed results. Several studies have actually reported decreased sperm counts following surgical weight loss, potentially due to nutritional deficiencies, rapid hormonal shifts, or the metabolic stress of dramatic calorie restriction (Carette et al., 2019). A 2025 systematic review in Human Reproduction Update confirmed that improvements following lifestyle interventions were more consistent than those following bariatric surgery (HRU, 2025).
Bottom line: Hormonal improvements (increased testosterone, decreased oestradiol) begin within weeks of dietary weight loss. Sperm parameters can improve within 8–14 weeks, particularly with a structured programme. But the key is sustained weight loss — the improvements are maintained only if the weight stays off. Gradual, lifestyle-based weight loss is preferable to extreme surgical intervention from a fertility standpoint.
Exercise: 3–6 Months of Moderate Activity
Physical activity has a well-documented relationship with sperm quality, but it follows an inverted U-shaped curve — moderate exercise helps, but excessive high-intensity training can actually harm fertility.
A 2025 network meta-analysis of 14 RCTs with 1,079 subjects found that moderate-intensity exercise interventions lasting 3–6 months significantly improved sperm parameters. Specifically, 150–300 minutes per week of moderate exercise increased sperm concentration by 12–17% and viability by 8–10% (Song et al., 2025).
Outdoor aerobic exercise showed the strongest evidence for improving sperm volume, while indoor aerobic and resistance training were most effective for sperm motility.
A separate meta-analysis of RCTs established a significant association between physical activity and improvements in sperm concentration, total motility, total count, and normal morphology, as well as increased pregnancy and live birth rates (Lo Giudice et al., 2024).
The FASt randomised controlled trial in Italy demonstrated that a 4-month Mediterranean diet combined with moderate physical activity improved sperm concentration, motility (total and progressive), and normal morphology in healthy young men — even those living in highly polluted areas (Montano et al., 2022; Donato et al., 2025).
Important caveats:
Excessive exercise is counterproductive. More than 10 hours per week of vigorous exercise may decrease sperm concentration by 14–20% and damage sperm DNA integrity through increased oxidative stress (Song et al., 2025).
Cycling deserves special mention. Prolonged cycling can increase scrotal temperature and compress the perineum. If you cycle, consider padded shorts, standing on pedals regularly, and keeping sessions moderate.
Bottom line: Aim for 150–300 minutes per week of moderate exercise (brisk walking, jogging, swimming, light resistance training) sustained for 3–6 months. This is one of the best-supported lifestyle interventions and carries obvious benefits beyond fertility.
Heat Exposure Removal: 3–6 Months
Sperm production requires temperatures 2–4°C below core body temperature, which is why the testes sit outside the body in the scrotum. Sources of excess heat — hot tubs, saunas, tight underwear, laptops on laps, prolonged sitting, and certain occupations — can significantly impair spermatogenesis.
The encouraging news is that heat-related damage is highly reversible once the source is removed.
Sauna exposure
A carefully designed longitudinal study exposed 10 normozoospermic men to Finnish sauna (80–90°C, 15 minutes, twice weekly) for 3 months. At the end of the exposure period, sperm count and motility were strongly impaired, with significant alterations to chromatin structure and mitochondrial function. However, all effects were completely reversed by 6 months after stopping sauna use (Garolla et al., 2013).
Experimental scrotal heating
A prospective study using controlled 43°C water-bath exposure confirmed reversible decreases in sperm concentration, motility, and function within a 16-week recovery period (Wu et al., 2015).
A pilot study that induced mild testicular temperature increases found that sperm aneuploidy (chromosomal abnormalities) doubled during the exposure period but was completely reversed at 180 days (6 months) post-exposure — suggesting that full recovery requires at least two cycles of spermatogenesis (Mieusset et al., 2019).
Hot tubs and baths
A study specifically looking at infertile men with a history of hot tub, Jacuzzi, or hot bath use found that 45% showed a mean 491% increase in total motile sperm count after cessation of the heat exposure (Shefi et al., 2007). Interestingly, the men who didn't respond tended to be smokers, suggesting that multiple insults make recovery harder.
Bottom line: Stop the heat exposure and wait 3–6 months. Most men see full recovery of conventional parameters within this window. Remove laptops from your lap, switch from tight to loose underwear, avoid hot tubs and prolonged hot baths, and take breaks from prolonged sitting. These are among the simplest and most effective changes you can make.
Varicocelectomy: Peak Improvement at 3 Months
A varicocele — an enlargement of the veins within the scrotum — is found in approximately 15% of all men and 40% of infertile men. Microsurgical repair is the most common surgical intervention for male infertility.
A landmark meta-analysis of 351 studies found that varicocelectomy produced a mean improvement of 9.7% in progressive motility and significant improvements in total motility and sperm concentration (Defined meta-analysis, 2023).
But the timing data is particularly interesting. A study that specifically investigated the optimal waiting period after varicocelectomy compared semen parameters at 3 and 6 months post-surgery. The finding? Maximum improvement occurred by 3 months, with no significant additional benefit between 3 and 6 months (Ghaed et al., 2020).
This makes sense when you consider the spermatogenesis cycle — one full cycle of new sperm, developed entirely under improved testicular conditions (better blood flow, lower temperature, reduced oxidative stress), will have completed by roughly 3 months after surgery.
Bottom line: After varicocelectomy, repeat your semen analysis at 3 months. If you're seeing improvement, that's likely your peak benefit from the surgery alone. Further improvements at 6+ months are more likely attributable to any concurrent lifestyle or supplement interventions than to ongoing surgical benefit.
Anabolic Steroids & TRT Recovery: 4–24+ Months
This is the intervention with the longest and most unpredictable recovery timeline, and it's one we see asked about frequently.
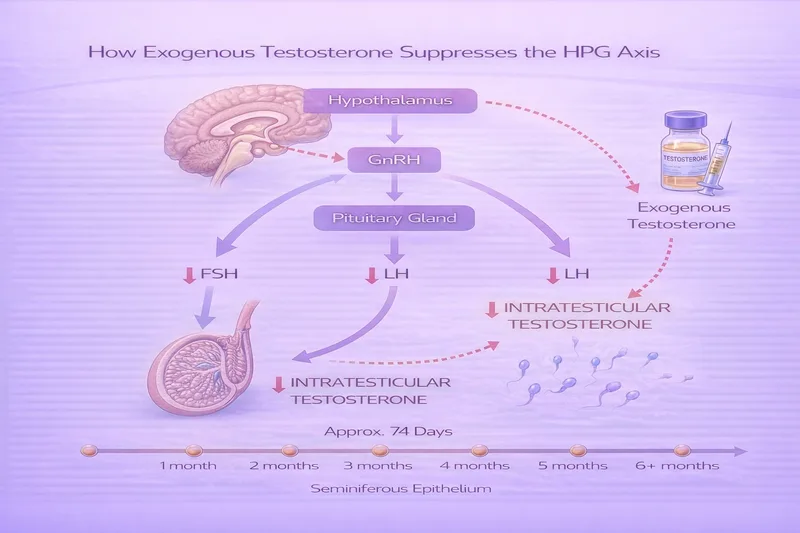
Both testosterone replacement therapy (TRT) and anabolic-androgenic steroids (AAS) suppress the hypothalamic-pituitary-gonadal (HPG) axis, shutting down natural testosterone and sperm production. The severity and duration of suppression depends on the drug(s) used, dose, duration, and individual factors.
What the evidence shows
A WHO contraceptive study of 271 healthy men receiving weekly testosterone injections found that mean time to recovery of sperm counts above 20 million/mL was 3.7 months after stopping, with all subjects reaching baseline levels at a mean of 6.7 months (WHO, 1990; cited in Avant et al., 2018).
A meta-analysis covering 30 clinical trials and over 1,500 men found 100% recovery to non-oligospermic levels within 2 years across varying contraceptive protocols (cited in Avant et al., 2018).
However, these were controlled medical studies with pharmaceutical-grade testosterone at moderate doses. Real-world AAS abuse is a different picture:
Recovery from AAS is feasible within 4–12 months in most cases, although some patients require up to 24–30 months to return to sperm concentrations above 20 million/mL (Wenker et al., 2017; cited in PMC, 2016).
A study specifically looking at AAS users who underwent 3 months of post-cycle therapy (PCT) found that HPG axis function recovered in 79.5% of cases — meaning roughly 1 in 5 men hadn't recovered even with medical assistance at 3 months (Shoskes et al., 2020).
Factors that delay recovery
Longer duration of use — Less than 1 year of use generally allows HPG axis recovery within 1 year of cessation. Longer use carries greater risk of delayed or incomplete recovery (Desai et al., 2022).
Multiple compounds ("stacking") — Using several AAS simultaneously causes deeper suppression.
Older age — The HPG axis becomes less resilient with age.
No post-cycle therapy — Medications such as clomiphene citrate or hCG can accelerate recovery by stimulating the pituitary or testes directly.
Recovery order
Spermatogenesis recovery follows a characteristic sequence: concentration recovers first, followed by motility, then morphology, with fertility potential typically being the last to fully normalise (PMC, 2023).
Bottom line: If you're on TRT or have used anabolic steroids and want to conceive, stop immediately and see a fertility specialist. Do not attempt unsupervised "PCT" — medical guidance with clomiphene, hCG, or FSH can significantly accelerate recovery. Expect 4–12 months for most cases, but budget for the possibility of 12–24+ months. For a more detailed discussion, see our low sperm motility article.
Alcohol Reduction: 3+ Months
The evidence on alcohol and sperm quality is somewhat dose-dependent. Moderate alcohol consumption (under 14 units per week) shows inconsistent effects in studies, but heavy drinking clearly disrupts the HPG axis, increases oxidative stress, and impairs liver metabolism of sex hormones.
There are fewer studies specifically tracking sperm recovery after alcohol cessation compared with smoking, but the biological principles are the same — one full spermatogenesis cycle (74+ days) is the minimum window for new, unaffected sperm to be produced.
Heavy alcohol use has cumulative effects with other insults, particularly smoking. If you're addressing both simultaneously, the combined benefit is likely greater than either alone.
Bottom line: Reduce intake to under 14 units per week (NHS guidelines) and allow at least 3 months to see results. If you're a heavy drinker, earlier improvements in hormonal markers may be seen, but full spermatogenesis recovery takes the standard 3-month minimum.
Medication Changes: Highly Variable
Several common medications can impair sperm quality:
SSRIs (antidepressants) — May increase sperm DNA fragmentation. Recovery timeline after discontinuation or switching is not well characterised but is likely within one spermatogenic cycle (3 months). Never stop antidepressants without medical guidance.
Finasteride (hair loss/prostate) — Can reduce sperm count and motility in some men. Most studies show recovery within 3–6 months of stopping, though rare cases of prolonged effects have been reported.
Chemotherapy — Recovery timeline is highly drug-dependent and dose-dependent. Some men recover spermatogenesis within 12 months, while others experience permanent impairment. Sperm banking before treatment is strongly advised.
Bottom line: Any medication changes should be discussed with your prescriber and ideally a fertility specialist. The timeline depends entirely on the specific drug and your individual response.
What to Do With These Timelines: A Practical Plan
Understanding these timelines helps you structure your approach and set realistic expectations. Here's a suggested framework:
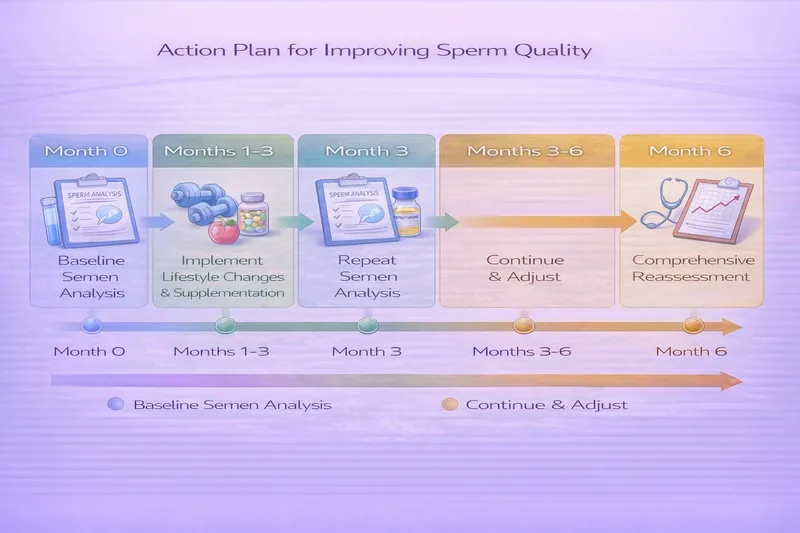
Month 0: Baseline
Get a comprehensive semen analysis. This is your starting point. If results are abnormal, your GP should repeat the test after 2–4 weeks (as there's a natural 28–43% variation between samples).
Identify your modifiable risk factors — smoking, weight, heat exposure, supplements you're not taking, exercise you're not doing.
Months 1–3: Implement Everything Simultaneously
Don't stagger your interventions. Since you're going to wait at least 3 months regardless, start everything at once:
Stop smoking completely. This is the single most impactful lifestyle change.
Start an evidence-based supplement stack. The strongest evidence supports L-carnitine (2g) + L-acetyl carnitine (1g) + CoQ10 (200–400mg) daily. See our supplements guide for the full ranking.
Address weight. If your BMI is above 25, a structured dietary approach combined with moderate exercise (150–300 minutes per week) can begin improving hormonal profiles within weeks.
Remove heat sources. Switch to boxers, avoid hot baths/saunas, move your phone from your front trouser pocket, keep laptops off your lap.
Reduce alcohol to under 14 units per week, ideally less.
Get treated for any medical causes. If you have a varicocele, seek referral for assessment. If there's a suspected infection, get it treated with antibiotics. If you're on TRT or anabolic steroids, see a fertility specialist immediately.
Month 3: First Reassessment
Repeat your semen analysis. Compare with baseline. You should see improvement if you've genuinely implemented changes — particularly in concentration and volume if you've quit smoking, and in motility if you've started L-carnitine or CoQ10.
If you had varicocelectomy, this is your peak improvement window.
If results have improved but are still below the WHO thresholds (≥16 million/mL concentration, ≥42% total motility, ≥30% progressive motility), continue your protocol.
Month 6: Comprehensive Review
Repeat your semen analysis again. By now, two full spermatogenesis cycles have completed under your improved regime. Smoking cessation benefits should be fully realised. Supplement effects should be at or near maximum.
If parameters have normalised — fantastic. Continue your healthy habits while trying to conceive.
If parameters haven't improved sufficiently, this is the point to escalate to a fertility specialist (reproductive urologist or andrologist) for:
Advanced testing (DNA fragmentation, oxidative stress markers, hormonal panel)
Consideration of assisted reproduction (IUI, IVF, or ICSI depending on severity)
Investigation of genetic or structural causes
Month 12+: Specialist-Led Management
If you've been trying to conceive for 12 months (or 6 months if your partner is over 35) without success despite improved semen parameters, seek fertility clinic referral. Both partners should be evaluated. See our when to see a fertility doctor guide for UK-specific NHS and private pathways.
Why Your First Repeat Test Might Look Worse (And Why That's OK)
Here's something that catches many men off guard: your first follow-up semen analysis after starting interventions sometimes looks worse than baseline. This doesn't necessarily mean your changes aren't working.
Semen analysis has significant natural variation — the same man can produce results that differ by 28–43% between samples even with no intervention at all (WHO, 2021). A single "worse" result on your first follow-up may simply reflect this normal variation, different abstinence periods, stress on the day, or laboratory variability.
This is why fertility specialists recommend at least two abnormal results before diagnosing a genuine problem, and why tracking the trend across multiple tests matters more than any single number.
Frequently Asked Questions
Can sperm quality improve after 40?
Yes, though the baseline trajectory at this age is a gradual decline. All the lifestyle and supplement interventions discussed here still work for men over 40 — you're fighting against a slightly steeper slope, but the principles are identical. Age-related decline is primarily in motility and DNA integrity rather than count.
Do I need to do everything on this list?
No. Focus on the factors that are relevant to you. If you don't smoke, smoking cessation won't help you. If your BMI is healthy, weight loss isn't your lever. But if you have multiple risk factors, addressing them simultaneously maximises your chances within the same 3-month window.
I've been trying supplements for 6 months with no improvement — now what?
If lifestyle changes and supplementation haven't produced meaningful improvement after 6 months, you're likely dealing with something that won't respond to these interventions alone — potentially a genetic cause, structural issue, or hormonal imbalance that needs medical investigation. Request referral to a reproductive urologist.
How often should I repeat my semen analysis?
Every 3 months while you're actively trying to improve parameters. More frequent testing (monthly, for example) creates unnecessary anxiety and is unlikely to show meaningful changes given the 74-day spermatogenesis cycle.
Should I avoid ejaculation to "save up" sperm?
Counterintuitively, very long abstinence periods (more than 5 days) actually decrease motility and increase DNA fragmentation. The optimal abstinence period before a semen analysis — and for conception attempts — is 2–5 days (WHO, 2021).
My partner is about to start IVF. Is it still worth me making changes?
Absolutely. Even with IVF or ICSI, better sperm quality improves fertilisation rates, embryo quality, implantation, and live birth rates. Start immediately — even 6–8 weeks of supplement use can begin improving the oxidative environment in seminal fluid before full spermatogenesis improvements kick in.
Can stress affect how quickly sperm quality improves?
Yes. Chronic stress elevates cortisol, which directly suppresses testosterone production via the HPG axis. It also tends to drive secondary behaviours — poor sleep, alcohol use, poor diet — that compound the problem. Stress management techniques won't directly improve sperm parameters, but they remove a significant barrier to improvement.
The Key Takeaway
Improving sperm quality is not instant, but it is achievable and evidence-based. The 74-day spermatogenesis cycle sets the minimum timeline, with most men seeing meaningful improvements within 3–6 months of sustained lifestyle, supplement, and/or medical interventions.
Start everything at once, commit to at least 3 months before assessing progress, and use repeat semen analyses to track your trend rather than obsessing over any single result. If 6 months of concerted effort hasn't produced improvement, that's valuable diagnostic information too — it tells you and your specialist where to focus next.
You're not powerless in this process. The evidence says otherwise.
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult your GP or a fertility specialist before starting supplements or making medication changes. If you've been trying to conceive for 12 months without success (6 months if your partner is over 35), seek professional evaluation.
Related articles:
- Understanding Semen Analysis Results: A Complete UK Guide
- Male Fertility Supplements UK: Evidence-Based Guide 2026
- Low Sperm Motility: Causes, Treatment & What Actually Helps
- Prenatal Vitamins UK: What You Actually Need When Trying to Conceive


