If you're trying to conceive (TTC), chances are you've been on the receiving end of well-meaning but frustrating advice: "Just relax and it'll happen!" or "You're stressing too much—that's why you're not pregnant." And if you're not pregnant yet, you might be lying awake at night wondering: Is my stress actually preventing me from conceiving?
Here's the truth: the relationship between stress and fertility is far more complicated than most people realize. The research doesn't support the simplistic "stress causes infertility" narrative, but it also doesn't mean stress has zero impact on your body.
This guide separates evidence from oversimplification, explains what stress actually does to your reproductive system, and—most importantly—why blaming yourself for being stressed is neither accurate nor helpful.
What the Research Actually Says
When you search "stress and fertility," you'll find conflicting information. Some sources claim stress is a major fertility blocker, while others say it has no impact at all. The reality sits somewhere in between, and understanding why the research is mixed is important.
The Nuanced Truth
What we know:
- Severe physiological stress (such as significant weight loss, extreme athletic training, major illness, or trauma) is known to disrupt ovulation in some women.
- Moderate, everyday stress has not consistently been shown to prevent pregnancy
- Acute stress (a bad day, an argument) doesn't stop you from conceiving
- The relationship is complex and varies between individuals
What we don't know:
- Exactly how much stress is "too much" for fertility
- Which women are most susceptible to stress-related fertility effects
- Whether treating stress alone improves conception rates
The Major Studies on Stress and Fertility
Let's look at what actual research shows—not headlines or anecdotes.
Study 1: Biomarkers of Stress and Time to Pregnancy (2014)
A prospective cohort study published in Human Reproduction followed 373 women who were trying to conceive and measured stress biomarkers in saliva, including cortisol and alpha-amylase.
Findings:
- Women with higher levels of alpha-amylase (a biomarker linked to stress) had a lower probability of conceiving in a given cycle.
- The reduction in fecundability was modest and primarily observed in women with the highest alpha-amylase levels.
- Salivary cortisol was not associated with reduced fertility.
- As an observational study, it could not establish whether stress caused reduced fertility or whether difficulty conceiving increased stress.
What this means:
Biological markers of higher stress were associated with slightly longer time to pregnancy in this study, but the effect was modest and does not prove that everyday stress prevents conception.
Study 2: Perceived Stress and Fecundability (2018)
A large prospective cohort study published in the American Journal of Epidemiology followed nearly 4,800 women in North America who were actively trying to conceive. The researchers measured perceived stress using a standardized scale and examined its relationship with fecundability — the probability of conceiving per cycle.
Findings:
- Higher perceived stress scores were associated with a modestly lower probability of conception per cycle.
- The association was small in magnitude.
- The study was observational and cannot prove causation.
- It was not designed to show that short-term or day-to-day stress directly prevents pregnancy.
What this means:
Higher perceived stress was associated with slightly longer time to pregnancy in this cohort, but the effect was modest and does not support the claim that normal everyday stress is a primary cause of infertility.
Study 3: Daily Stress and Conception (Prospective Cohort Data)
Some prospective cohort research examining daily perceived stress has not found a clear or consistent reduction in conception probability.
Findings:
- Day-to-day perceived stress was not consistently associated with reduced fecundability.
- The relationship between stress and fertility varies depending on how stress is measured (self-report vs biological markers).
- Clinical depression or anxiety disorders may show modest associations with reduced fertility in some studies, though mechanisms remain unclear.
What this means:
The broader research landscape suggests that while very high or chronic stress may be associated with slightly reduced fertility in some women, everyday fluctuations in stress do not consistently prevent pregnancy.
The Bottom Line from Research
Severe, chronic stress (ongoing for months, affecting sleep, eating, daily function) may reduce fertility for some women, but the effect is:
- Modest (not a major cause of infertility)
- Variable (doesn't affect everyone equally)
- Often confounded by other factors
Moderate, everyday stress (work deadlines, traffic, arguments) shows little to no consistent effect on fertility in most studies.
The "just relax" myth is not supported. No study has shown that simply relaxing or reducing mild stress significantly improves conception rates for women with no other fertility issues.
How Stress Could Affect Fertility (Biologically)
Even though the evidence is mixed, there are plausible biological mechanisms by which chronic stress might impact fertility.
1. Stress Hormones and Ovulation
How it works:
Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, releasing cortisol and other stress hormones. In theory, high cortisol can interfere with the hypothalamic-pituitary-ovarian (HPO) axis—the hormonal communication system that controls ovulation.
The evidence:
Some research shows that extreme stress (e. g., severe illness, famine, intense athletic training) can disrupt or delay ovulation. However, most everyday stress doesn't reach this threshold.
What this means:
In conditions of significant physiological stress, ovulation can be delayed or suppressed through hypothalamic mechanisms. This is well documented in conditions such as hypothalamic amenorrhea.
2. Cortisol and Reproductive Hormones
How it works:
Chronic high cortisol can theoretically suppress luteinizing hormone (LH) and follicle-stimulating hormone (FSH), both essential for ovulation.
The evidence:
Mixed. Some studies find correlations between cortisol and fertility, others don't. The relationship isn't straightforward, and cortisol fluctuates throughout the day, making it hard to measure accurately.
What this means:
If you're experiencing severe, chronic stress affecting your entire life (not sleeping, not eating, panic attacks), it's worth discussing with your GP. But if you're functioning normally despite feeling stressed about TTC, your cortisol probably isn't the problem.
3. Behavioral Effects of Stress
This is often overlooked but may be more significant than hormonal effects.
How it works:
Stress can lead to:
- Reduced libido (less sex during fertile window)
- Irregular eating or sleeping patterns
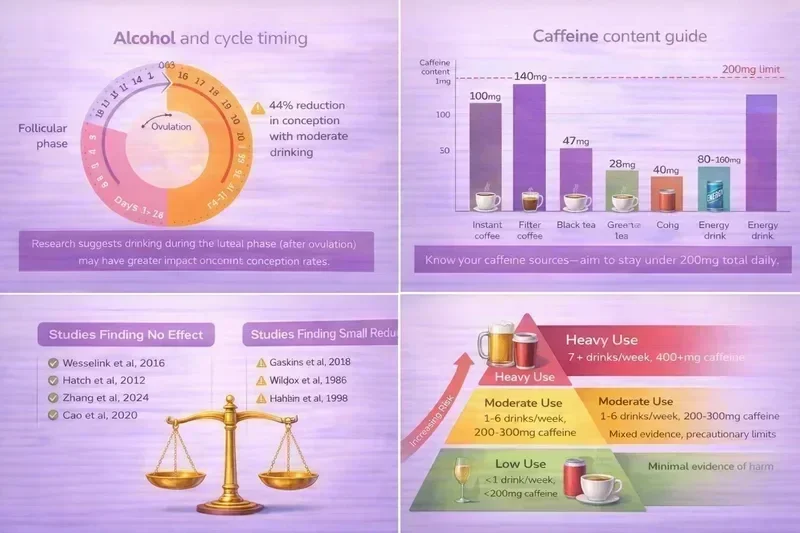
- Increased alcohol or caffeine intake
- Avoiding social situations (like intimacy)
The evidence:
Several studies suggest that stress's impact on behavior (particularly sexual activity) may explain much of the stress-fertility link.
What this means:
In many studies, behavioural factors such as intercourse frequency appear to explain more of the stress–fertility association than direct hormonal suppression. This is actionable—you can make an effort to prioritize intimacy even when stressed.
Why "Just Relax" Is Terrible Advice
You've probably heard some version of:
- "Just relax and it'll happen!"
- "Stop stressing—that's why you're not pregnant."
- "My friend stopped trying and got pregnant immediately!"
- "Take a vacation—you'll come back pregnant!"
This advice is not only unsupported by evidence—it's actively harmful.
1. It Blames the Person Struggling to Conceive
Telling someone their stress is preventing pregnancy implies:
- You're doing this to yourself
- If you just tried harder to relax, you'd be pregnant
- Your inability to control stress is the problem
This creates a vicious cycle: you're stressed about not conceiving, then stressed about being stressed, then stressed that your stress-about-stress is preventing pregnancy. It's unhelpful and cruel.
2. It Dismisses Legitimate Fertility Concerns
If you've been trying for 6-12 months without success, the appropriate response isn't "just relax"—it's to see your GP for fertility testing.
Conditions like PCOS, endometriosis, blocked fallopian tubes, low sperm count, or thyroid issues don't resolve by "relaxing." Delaying medical evaluation because you think you're "too stressed" wastes valuable time.
The NHS recommends seeking fertility advice after:
- 12 months of trying (if under 35)
- 6 months of trying (if over 35)
Stress isn't mentioned as a reason to delay seeking help.
3. It Oversimplifies a Complex Issue
Fertility depends on dozens of factors:
- Age
- Ovulation regularity
- Sperm quality
- Fallopian tube health
- Uterine health
- Timing of intercourse
- Underlying medical conditions
Stress is, at most, one small piece of a complex puzzle. Reducing it to "just relax" ignores all the other factors.
4. It's Not Evidence-Based
No study has shown that relaxation techniques, meditation, or stress reduction programs significantly improve conception rates for women with no other fertility issues.
Some research suggests stress reduction may help women undergoing IVF (possibly by improving adherence to treatment protocols), but for natural conception, the evidence is weak.
When Stress IS Worth Addressing
While everyday stress probably isn't preventing pregnancy, there are scenarios where stress management is important for your wellbeing—regardless of its impact on fertility.
1. Stress Is Affecting Your Quality of Life
If stress is:
- Preventing you from sleeping
- Causing panic attacks or constant anxiety
- Affecting your relationships
- Making you withdraw from activities you enjoy
- Impacting your work or daily functioning
You deserve support—not because it'll make you pregnant, but because your mental health matters.
The NHS provides mental health services including free talking therapies. You don't need to be in crisis to access support.
2. You Have a Diagnosed Mental Health Condition
Clinical depression and anxiety are different from everyday stress.
If you have:
- Major depressive disorder
- Generalized anxiety disorder
- PTSD
- Panic disorder
- OCD
Some research suggests these conditions may modestly affect fertility, though the mechanisms aren't fully understood. More importantly, these conditions affect your quality of life and are treatable.
Speak to your GP about:
- Therapy (CBT, counselling)
- Medication (some antidepressants are safe during TTC and pregnancy)
- Support groups
Treat your mental health because it matters, not just because you want to conceive.
3. Stress Is Changing Your Behavior
If stress is causing you to:
- Avoid sex during your fertile window
- Skip tracking ovulation because it's "too stressful"
- Drink heavily or use substances to cope
- Stop taking care of your physical health
These behaviors could indirectly affect fertility. Managing stress to improve these behaviors is worthwhile.
Practical Stress Management for TTC (Evidence-Based)
If you want to manage stress—for your wellbeing, not as a fertility treatment—here's what has some evidence behind it.
1. Maintain Regular Sleep
Why it matters:
Sleep deprivation increases cortisol and affects hormonal balance generally. While it's not proven to prevent pregnancy, chronic sleep deprivation is unhealthy.
What to do:
- Aim for 7-9 hours per night
- Keep a consistent sleep schedule
- Limit screen time before bed
- Avoid caffeine after 2pm
2. Physical Activity
Why it matters:
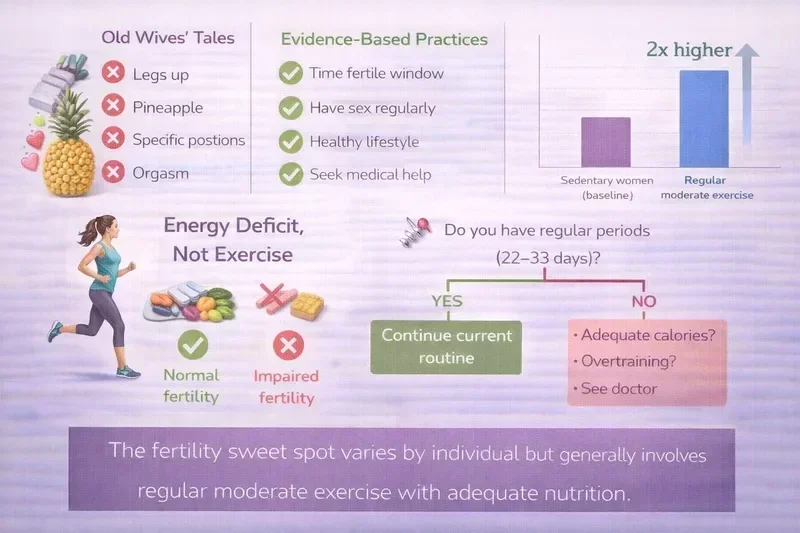
Exercise reduces stress hormones and improves mood. Moderate exercise is associated with better fertility outcomes (though extreme exercise can disrupt cycles).
What to do:
- 30 minutes of moderate activity most days (walking, swimming, yoga, cycling)
- Avoid over-exercising (>7 hours of intense cardio per week can affect ovulation)
- Choose activities you enjoy, not punishment-style workouts
See our article: Pregnancy Exercise Myths: Can You Really Harm Your Baby Working Out?
3. Social Connection
Why it matters:
Isolation increases stress. Social support improves resilience and mental health.
What to do:
- Stay connected with friends and family (even when TTC feels all-consuming)
- Consider joining a TTC support group (online or in-person)
- Don't isolate yourself because pregnancy announcements are painful—find people who understand
UK resources:
- Fertility Network UK - Support groups and forums
4. Limit Obsessive Tracking
Why it matters:
Excessive cycle tracking (testing 10 times per day, charting every symptom, googling constantly) can increase anxiety without improving conception chances.
What to do:
- Track the essentials: period start date, ovulation (if using tests or BBT)
- Limit symptom spotting in the two-week wait
- Avoid testing for pregnancy before 12 days past ovulation
- Set boundaries on TTC-related internet searching
See our guide: How to Track Ovulation When Trying to Conceive: Complete UK Guide 2026
5. Therapy or Counselling
Why it matters:
Talking to a professional can help you process the emotions around TTC without judgment.
What to do:
- Ask your GP about NHS talking therapies
- Consider fertility counselling (some fertility clinics offer this)
- Private therapy if you prefer (BACP-registered counsellors)
This isn't about "relaxing to get pregnant"—it's about coping with a difficult experience.
6. Mindfulness or Meditation (If You Want To)
Why it matters:
Some people find mindfulness helpful for managing anxiety. The evidence for fertility benefits is weak, but it won't hurt.
What to do:
- Try apps like Headspace, Calm, or Insight Timer
- Fertility-specific meditation apps exist but aren't proven more effective
- If it helps you feel better, great. If it stresses you out, skip it.
Don't force yourself to meditate because you think it'll make you pregnant. There's no evidence for that.
What Actually Prevents Pregnancy (It's Not Stress)
If you're not conceiving, stress is unlikely to be the primary cause. Here are the most common actual reasons:
1. Not Timing Intercourse Correctly
The issue:
You can only get pregnant during the ~6-day fertile window ending on ovulation day. If you're not having sex during this window, you won't conceive—regardless of stress levels.
The solution:
Track ovulation using LH tests, cervical mucus, or apps. Have sex every 1-2 days during the fertile window.
See our guides:
- Understanding Your Menstrual Cycle When Trying to Conceive: UK Guide
- Best Ovulation Tests UK 2026: Reviews for Trying to Conceive
2. Irregular or Absent Ovulation
The issue:
Conditions like PCOS, thyroid disorders, or hypothalamic amenorrhea can prevent ovulation. No ovulation = no pregnancy.
The solution:
See your GP for blood tests to confirm ovulation. Treatment (e. g., Clomid for PCOS) can restore ovulation.
3. Age-Related Fertility Decline
The issue:
Fertility declines with age, particularly after 35. Egg quality and quantity decrease.
The solution:
Seek fertility advice sooner if you're over 35 (after 6 months of trying). Consider fertility testing.
The NHS provides information on age and fertility.
4. Male Factor Infertility
The issue:
About 30-40% of infertility cases involve male factors (low sperm count, poor motility, abnormal morphology).
The solution:
Your partner needs a semen analysis. This is simple, non-invasive, and available through your GP.
5. Structural Issues
The issue:
Blocked fallopian tubes, endometriosis, fibroids, or uterine abnormalities can prevent conception.
The solution:
Fertility testing (ultrasound, hysterosalpingography) can identify these issues. Many are treatable.
When to See Your GP
Don't wait to seek fertility help because you think you're "too stressed."
The NHS recommends seeing your GP if:
You're under 35:
After 12 months of regular, unprotected intercourse without conceiving
You're 35 or older:
After 6 months of regular, unprotected intercourse without conceiving
You have known risk factors:
- Irregular or absent periods
- PCOS, endometriosis, or thyroid issues
- History of pelvic infections or surgery
- Your partner has known fertility concerns
Your GP can:
- Confirm you're ovulating (blood tests)
- Arrange semen analysis for your partner
- Check for underlying conditions (PCOS, thyroid)
- Refer you to NHS fertility services if needed
Stress alone is not considered a reason to delay medical evaluation. NHS guidance recommends fertility assessment after 12 months (or 6 months if over 35), regardless of stress levels.
The Stress-Infertility Cycle
Here's the real problem with the stress-fertility narrative:
1. You struggle to conceive (for any number of reasons—age, PCOS, timing, sperm issues, etc.)
2. You become stressed (understandably—it's disappointing and frustrating)
3. Someone tells you "You're too stressed—that's why you're not pregnant"
4. You become stressed about being stressed ("I need to relax or I'll never get pregnant")
5. You blame yourself for not being able to "just relax"
6. This increases stress and delays you seeking actual medical help
This cycle is harmful. The solution isn't to eliminate stress (impossible for most people)—it's to recognize that stress is a normal response to a difficult situation, not the cause of the difficulty.
Reframing Stress and TTC
Instead of:
"I need to stop being stressed or I'll never get pregnant."
Try:
"It's normal to feel stressed when trying to conceive. I'll manage my stress because my mental health matters, not because I think it's preventing pregnancy."
Instead of:
"I should just relax and it'll happen."
Try:
"I've been trying for [X] months. I'll see my GP to rule out medical issues while also taking care of my mental health."
Instead of:
"Everyone tells me to relax, so stress must be my problem."
Try:
"The research on stress and fertility is mixed. I'll focus on what I can control: timing intercourse, tracking ovulation, and seeking medical advice if needed."
Final Thoughts
If you take one thing from this article, let it be this:
For most people, everyday stress is unlikely to be the primary reason pregnancy has not occurred
Trying to conceive is inherently stressful for many people. Month after month of hope followed by disappointment is emotionally exhausting. It's normal to feel anxious, frustrated, sad, or overwhelmed. Feeling these emotions doesn't mean you're doing something wrong or sabotaging your chances.
The evidence suggests that extreme, chronic stress might have a modest impact on fertility for some women, but everyday stress—even significant everyday stress—is unlikely to be the primary reason you're not conceiving.
If you're struggling with stress, seek support because your mental health and quality of life matter—not because you think managing stress will magically make you pregnant.
And if you've been trying for 6-12 months without success, see your GP for fertility testing. Many fertility issues are treatable, but they don't resolve by "just relaxing."
You deserve compassionate, evidence-based support—not blame.

Related Articles
- "Just Relax" Fertility Myth
- Understanding Your Menstrual Cycle When Trying to Conceive
- How to Track Ovulation When Trying to Conceive
- Exercise Myths When TTC: How Much Is Too Much?
- When to See a Fertility Doctor UK: Guide for Trying to Conceive
Note on Research Citations: This article combines NHS guidance with peer-reviewed research from leading medical journals. All citations are linked directly in the text for verification.
It’s also important to recognise that infertility itself can increase stress, making it difficult to determine direction of effect in observational research.
Disclaimer: This article provides evidence-based information about stress and fertility. It is not a substitute for medical or mental health advice. If you're struggling with anxiety, depression, or difficulty conceiving, please consult your GP or a mental health professional.