
When you're trying to conceive (TTC), understanding your menstrual cycle transforms from something you vaguely tracked for period prediction into essential knowledge for timing intercourse and maximizing your chances of pregnancy.
But here's what many women don't realize: the textbook 28-day cycle with ovulation on day 14 is far less common than most people think. Real-world data shows only around 13% of cycles are exactly 28 days — and even those don’t always follow the ‘day 14’ rule.
This guide explains how your menstrual cycle actually works, how to identify your fertile window regardless of cycle length, and when cycle irregularities warrant a conversation with your GP.
The Four Phases of Your Menstrual Cycle
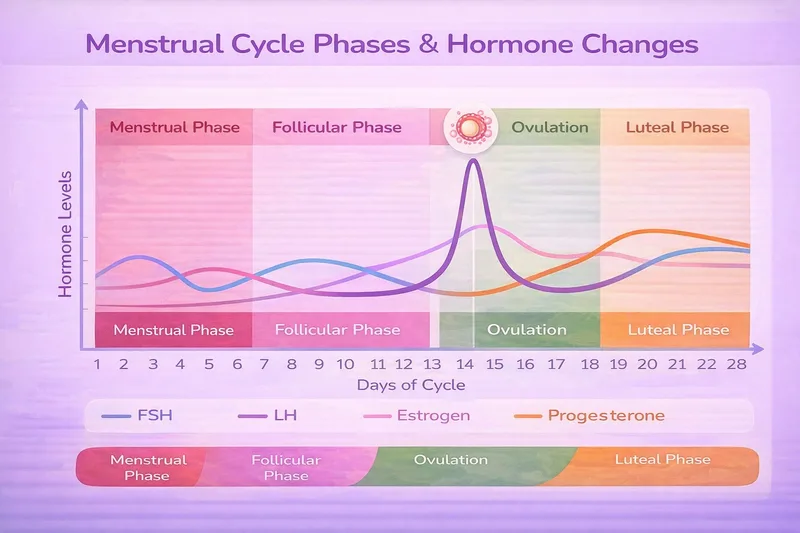
Your menstrual cycle is controlled by a complex interplay of hormones that prepare your body for potential pregnancy each month. Understanding what happens during each phase helps you identify when you're most fertile.
Phase 1: Menstruation (Days 1-5)
What's happening:
Your period marks the beginning of your cycle. When pregnancy doesn't occur, falling progesterone levels trigger the shedding of your uterine lining (endometrium), which exits your body as menstrual blood.
Hormones: Estrogen and progesterone are at their lowest levels.
Duration: Typically 3-7 days, though 2-7 days is still considered normal by the NHS.
Fertility: Usually low. Pregnancy from sex during your period is unlikely, but it can happen — especially if you ovulate soon after your period ends and sperm survive several days.
What you might notice:
- Bleeding (light to heavy)
- Cramping or pelvic discomfort
- Lower energy levels
- Mood changes
Phase 2: Follicular Phase (Days 1-13, approximately)
What's happening:
This phase overlaps with menstruation and continues until ovulation. Your pituitary gland releases follicle-stimulating hormone (FSH), which signals your ovaries to develop several follicles—tiny sacs that each contain an immature egg. Usually, one dominant follicle continues to develop while the others stop growing.
Hormones: Estrogen levels gradually rise as the dominant follicle matures and produces estrogen.
Duration: Variable (7-21 days). This is the phase that varies most between women and from month to month, determining your overall cycle length.
Fertility: Low initially, then increasing as you approach ovulation.
What you might notice:
- Energy levels increase
- Cervical mucus becomes more abundant and changes from dry/sticky to creamy
- Mood may improve (estrogen's effect)
- Increased libido as ovulation approaches
Why this matters for TTC:
The length of your follicular phase determines when you ovulate. A woman with a 24-day cycle might ovulate on day 10, while someone with a 34-day cycle might ovulate on day 20—not the mythical day 14.
Phase 3: Ovulation (Day 14-ish, but often not!)
What's happening:
Rising estrogen levels trigger a surge in luteinising hormone (LH) from your pituitary gland. This LH surge causes the dominant follicle to rupture and release a mature egg—this is ovulation. The egg travels into the fallopian tube, where it can potentially be fertilized for 12-24 hours.
Hormones: LH surges 24-36 hours before ovulation. Estrogen peaks just before ovulation, then drops. Progesterone begins to rise.
Duration: Ovulation itself is a brief event (the egg is released), but the LH surge that triggers it lasts 12-48 hours.
Fertility: This is your peak fertility. Your fertile window includes the days leading up to ovulation because sperm can survive for several days after sex (the NHS notes up to 7 days in the fallopian tubes).
What you might notice:
- Egg white cervical mucus (EWCM): Clear, stretchy, slippery—this is the most reliable physical sign
- Mild pelvic pain or twinges on one side (mittelschmerz—ovulation pain)
- Increased libido
- Slight increase in basal body temperature (but this only confirms ovulation after it's already happened)
- Breast tenderness
- Some women notice light spotting
Why this matters for TTC:
This is your target window. The NHS explains that you're most fertile during the few days before and on the day you ovulate.
The science: A landmark study published in the New England Journal of Medicine tracked 625 women and found that nearly all pregnancies occurred when intercourse happened during a 6-day window ending on the day of ovulation, with the highest conception rates on the day before ovulation.
Phase 4: Luteal Phase (Days 15-28, approximately)
What's happening:
After releasing the egg, the ruptured follicle transforms into the corpus luteum, a temporary endocrine structure that produces progesterone. Progesterone thickens the uterine lining, creating a nutrient-rich environment for a fertilized egg to implant. If pregnancy occurs, the developing embryo produces hCG (human chorionic gonadotropin), which signals the corpus luteum to keep producing progesterone. If pregnancy doesn't occur, the corpus luteum breaks down after about 14 days, progesterone levels drop, and menstruation begins.
Hormones: Progesterone dominates. Estrogen rises again but remains lower than during ovulation.
Duration: Typically 12-16 days. Unlike the follicular phase, the luteal phase is relatively consistent for each individual woman. Most women have a luteal phase of 14 days (±2 days), though 10-16 days is considered normal.
Fertility: None. Once ovulation has passed, you cannot conceive until your next cycle.
What you might notice:
- Increased basal body temperature (0.2-0.5°C higher than follicular phase)
- Premenstrual symptoms (PMS): bloating, breast tenderness, mood changes, food cravings
- Cervical mucus becomes thick or dries up
- Energy levels may decrease
- If pregnant: no period, possible early pregnancy symptoms
Why this matters for TTC:
Tracking your luteal phase length helps you understand your cycle pattern. A consistently short luteal phase (under 10 days) can affect fertility and may warrant GP consultation.
What's a "Normal" Cycle Length?
The NHS defines a normal menstrual cycle as 21-35 days, measured from the first day of one period to the first day of the next.
Here's what this means:
Under 21 days: Short cycle—may indicate issues with ovulation or luteal phase
21-35 days: Most common range, considered regular
35–40 days: Longer cycles are common, but if your cycle is regularly over 35 days, the NHS classifies that as irregular and it can sometimes reflect less predictable ovulation.
Over 40 days or highly variable: More clearly irregular — common causes include PCOS, thyroid issues, stress, or weight changes.
Research confirms most women don't have the textbook 28-day cycle. A large study published in npj Digital Medicine analysing over 600,000 menstrual cycles found that only around 13% of cycles were exactly 28 days.. The average cycle length was 29.3 days, with normal variation ranging from 25-30 days for most women.
Your cycle is "regular" if:
- It varies by no more than 7-9 days from cycle to cycle
- You can generally predict when your period will arrive (give or take a few days)
- You have some consistency in pattern over 3-6 months
Your cycle may be "irregular" if:
- Length varies by 10+ days from month to month
- You can't predict when your period will come
- You frequently miss periods (fewer than 9 periods per year)
- Periods are very frequent (more than 13 periods per year)
The Day 14 Ovulation Myth
The myth: Everyone ovulates on day 14 of their cycle.
The reality: Even in women with 28-day cycles, ovulation does not consistently occur on day 14. Research shows that ovulation timing varies more than most people expect, which is why relying on a fixed “day 14” rule often leads to mistimed intercourse.
Here's why the myth exists:
Medical textbooks use a 28-day cycle as the "standard" example because it's mathematically convenient. In a perfect 28-day cycle with a standard 14-day luteal phase, ovulation would occur on day 14 (28 - 14 = 14). But most women don't have perfect 28-day cycles, and even those who do may have luteal phases of 12 or 16 days.
How to calculate YOUR ovulation day:
Step 1: Track your cycle length for 3-6 months.
Step 2: Assume your luteal phase is 14 days (this is more consistent than follicular phase).
Step 3: Subtract 14 from your average cycle length.
Examples:
- 24-day cycle: Likely ovulation on day 10 (24 - 14 = 10)
- 28-day cycle: Likely ovulation on day 14 (28 - 14 = 14)
- 32-day cycle: Likely ovulation on day 18 (32 - 14 = 18)
- 35-day cycle: Likely ovulation on day 21 (35 - 14 = 21)
This is an estimate. To know for certain, use ovulation tracking methods or ovulation predictor kits.
How to Identify Your Fertile Window
Your fertile window is the roughly 6-day period when pregnancy is possible: the 5 days before ovulation plus the day of ovulation itself.
Why 6 days?
Sperm can survive in the female reproductive tract for up to 5 days in fertile cervical mucus, but an egg only survives 12-24 hours after ovulation. This creates a narrow but crucial window.
Research confirms this timing: The same NEJM study found that nearly all pregnancies occur from intercourse during a six-day window ending on the day of ovulation. The highest conception rates are seen on the day before ovulation and the day of ovulation itself, with pregnancy still possible during the five days leading up to ovulation due to sperm survival.
Method 1: Calendar Calculation
Best for: Women with regular cycles
How it works:
- Track your cycles for 3-6 months to find your average length
- Subtract 14 to estimate ovulation day
- Count back 5 days to find the start of your fertile window
Example (30-day cycle):
- Estimated ovulation: Day 16
- Fertile window: Days 11-16
Limitation: This is an estimate. Your actual ovulation can vary by a few days each month.
Method 2: Cervical Mucus Monitoring
Best for: Women comfortable checking their bodies
How it works:
As ovulation approaches, rising estrogen changes your cervical mucus:
After period: Dry or minimal mucus (not fertile)
Mid-follicular phase: Sticky or creamy white mucus (low fertility)
Approaching ovulation: Wet, slippery mucus (fertility increasing)
Peak fertility: Clear, stretchy, slippery "egg white" mucus—EWCM (most fertile)
After ovulation: Mucus dries up or becomes thick and sticky again (not fertile)
Why this works:
Fertile cervical mucus helps sperm survive and travel to the egg. When you see EWCM, you're entering your most fertile days.
Method 3: Ovulation Predictor Kits (LH Tests)
Best for: Women who want precise timing
How it works:
Test strips or digital tests detect the LH surge that happens 24-36 hours before ovulation.
When to test: Start testing several days before you expect to ovulate (use the calendar calculation as a guide).
Result: When the test is positive, ovulation will occur within 12-48 hours—this is your signal to have intercourse.
See our complete guide: Best Ovulation Tests UK 2026: Reviews for Trying to Conceive
Method 4: Basal Body Temperature (BBT)
Best for: Confirming ovulation happened (retrospective)
How it works:
Your resting body temperature rises 0.2-0.5°C after ovulation due to progesterone.
Limitation: BBT only confirms ovulation after it's already happened, so it's best combined with cervical mucus monitoring or LH tests.
See our complete guide: How to Track Ovulation When Trying to Conceive: Complete UK Guide 2026
When Cycle Irregularities Matter
Some variation is normal. Most women experience the occasional early or late period due to stress, illness, travel, or unexplained factors.
When to see your GP:
1. Irregular periods (cycles vary by 10+ days)
Possible causes:
- Polycystic ovary syndrome (PCOS)—most common cause
- Thyroid disorders (hypo- or hyperthyroidism)
- Stress, excessive exercise, or significant weight loss
- Approaching perimenopause (if over 40)
Why it matters: Irregular cycles often indicate irregular or absent ovulation, making conception difficult.
What your GP can do: Blood tests to check hormone levels, pelvic ultrasound if needed, treatment options (e. g. Ovulation-induction medicines may be considered if appropriate.).
2. Very short cycles (under 21 days consistently)
Possible causes:
- Short follicular phase (rapid egg development)
- Short luteal phase (progesterone deficiency)
- Perimenopause
Why it matters: Short luteal phase (<10 days) may not allow enough time for embryo implantation.
What your GP can do: Progesterone blood tests in the luteal phase, treatment if needed.
3. Very long cycles (over 35-40 days consistently)
Possible causes:
- PCOS (most common)
- Hypothyroidism
- Hyperprolactinemia
- Stress or low body weight
Why it matters: Ovulation may be infrequent or absent.
What your GP can do: Hormone testing, ovulation induction medications if needed.
4. Missing periods (fewer than 9 periods per year)
Possible causes:
- Pregnancy (test first!)
- PCOS
- Significant weight loss or low BMI
- Excessive exercise
- Stress
- Early menopause (if under 40)
Why it matters: Absent periods usually mean absent ovulation—you can't conceive without ovulation.
NHS guidance: The NHS recommends seeing your GP if you've missed 3 or more periods in a row and aren't pregnant.
5. Very heavy or painful periods
Possible causes:
- Endometriosis
- Uterine fibroids
- Adenomyosis
- Pelvic inflammatory disease
Why it matters: These conditions can affect fertility and may require treatment.
What your GP can do: Pelvic examination, ultrasound, referral to gynecologist if needed. The NHS provides guidance on heavy periods and when to seek help.
When to See Your GP About Fertility
The NHS recommends seeking fertility advice if:
You're under 35:
After 12 months of regular, unprotected intercourse without conceiving
You're 35 or older:
After 6 months of regular, unprotected intercourse without conceiving
You have known risk factors:
- Irregular or absent periods
- History of pelvic infections or STIs
- Diagnosed endometriosis or PCOS
- Previous pelvic surgery
- Your partner has known fertility concerns
What your GP can offer:
- Initial fertility testing (blood tests to check ovulation, hormone levels)
- Semen analysis for your partner
- Referral to NHS fertility services if needed
- Treatment for underlying conditions affecting fertility
Don't wait if you're concerned: While the 6-12 month guidance is standard, you can speak to your GP sooner if you have irregular cycles or other fertility concerns.
See our guide: When to See a Fertility Doctor UK: Guide for Trying to Conceive
Your Cycle and Age
Cycle regularity changes with age:
In Your 20s
- Ovulation typically occurs regularly in early adulthood, and cycles tend to be more predictable in your 20s compared with later decades.
- Average cycle length: 27-29 days
In Your 30s
- Still regular for most women
- Slight decrease in ovulation frequency
- Cycle length may shorten slightly (1-2 days shorter by late 30s)
In Your 40s
- Increasing irregularity (perimenopause begins for some)
- Cycles may become longer, shorter, or unpredictable
- Ovulation becomes less frequent
The NHS notes that fertility naturally declines with age, particularly after 35, and cycle patterns often become less predictable in the years leading up to menopause.
Research confirms this: A study published in npj Digital Medicine analyzing over 165,000 menstrual cycles found that cycle variability is 46% higher in women aged 45–49 compared to those aged 35–39, with both the length and regularity of cycles becoming less predictable with age.
What this means for TTC:
If you're in your late 30s or 40s with irregular cycles, don't wait 12 months to seek fertility advice—speak to your GP sooner.
Common Questions About Cycles and TTC
Can I get pregnant during my period?
Unlikely, but possible in rare cases.
If you have very short cycles (21 days or less) and ovulate early (day 7-9), sperm from intercourse during your period could potentially survive long enough to fertilize the egg. For most women with regular cycles, period sex won't result in pregnancy.
See our article: Can You Get Pregnant on Your Period? What Science Actually Says
Why does my cycle length vary each month?
The follicular phase varies, the luteal phase usually doesn't.
Stress, illness, travel, weight changes, intense exercise, and even changes in sleep can affect how quickly your follicle develops, shifting ovulation earlier or later. Your luteal phase (after ovulation) tends to stay consistent.
A few days' variation (e. g., 28-31 days) is totally normal. Variation of 10+ days suggests irregular ovulation.
How long after stopping birth control will my cycle return to normal?
Depends on the type:
Combined pill or mini pill: Usually 1-3 months. Some women ovulate within weeks.
Hormonal IUD (Mirena): 1-6 months, though some women don't have periods on Mirena and may not notice a change.
Depo-Provera injection: Can take 6-18 months for ovulation to return.
Copper IUD (non-hormonal): Immediate—your natural cycle resumes right away.
The NHS provides information about planning pregnancy after stopping contraception.
See our article: Does the Pill Damage Fertility? Contraception Myths Debunked
Can stress delay ovulation?
Yes. Stress affects the hypothalamic-pituitary-ovarian axis—the hormonal communication system that controls your cycle.
High stress can delay ovulation (making your cycle longer) or occasionally prevent ovulation altogether (resulting in a missed period). Once ovulation occurs, the luteal phase proceeds normally.
See our article: Does Stress Prevent Pregnancy? What Science Says for Trying to Conceive
Should I track my cycle even if it's regular?
Yes, even with regular cycles, tracking helps you:
- Pinpoint your fertile window more accurately
- Notice any changes that might indicate a problem
- Gather data to share with your GP if needed
- Reduce anxiety by knowing what's happening in your body
You don't need expensive apps—a simple calendar noting period start dates and any symptoms (mucus, ovulation pain) is enough.
Putting It All Together: Your TTC Cycle Strategy
Week 1 (Menstruation):
- Track first day of period (this is cycle day 1)
- Note flow and duration
- Recovery/rest phase—no special TTC actions needed
Week 2 (Follicular Phase):
- Monitor cervical mucus (begins changing as ovulation approaches)
- If using ovulation tests, start testing a few days before expected ovulation
- Begin increasing intercourse frequency as fertile window approaches
Week 3 (Ovulation/Fertile Window):
- Watch for peak cervical mucus (EWCM)
- Positive ovulation test = ovulation within 12-48 hours
- Have intercourse every 1-2 days during fertile window
- Aim for the 2-3 days before ovulation plus ovulation day itself
Week 4 (Luteal Phase):
- If tracking BBT, watch for temperature shift confirming ovulation
- Wait for period or pregnancy test (test 12-14 days after ovulation)
- Try not to over-analyze symptoms ("symptom spotting" causes unnecessary stress)
Repeat each cycle, adjusting timing based on what you learn about YOUR unique pattern.
Final Thoughts
Your menstrual cycle is not a mystery or something that "just happens." It's a precise, hormone-driven process that you can understand and work with to maximize your chances of conception.
The key isn't following a generic "day 14" rule—it's learning YOUR body's unique rhythm. Whether your cycle is 25 days or 35 days, regular or slightly irregular, understanding the phases, recognizing your fertile signs, and timing intercourse accordingly gives you the best possible chance of conceiving.
And if something doesn't feel right—persistently irregular cycles, very short or long cycles, or difficulty conceiving after 6-12 months—don't hesitate to speak with your GP. Many cycle irregularities are treatable, and early intervention can make a significant difference.
Related Articles
- How to Track Ovulation When Trying to Conceive: Complete UK Guide
- Best Ovulation Tests UK 2026: Reviews for Trying to Conceive
- Can You Get Pregnant on Your Period? What Science Actually Says
- Ovulation Timing Myths: When Can You Actually Get Pregnant?
- Does the Pill Damage Fertility? Contraception Myths Debunked
Note on Research Citations: Medical studies referenced in this article are linked directly in the text. Click any study reference to read the original research from journals including Human Reproduction, BMJ, and The New England Journal of Medicine.
Disclaimer: This article provides educational information about menstrual cycles and fertility based on NHS guidance and peer-reviewed research. It is not a substitute for medical advice. If you have concerns about your menstrual cycle, irregular periods, or difficulty conceiving, please consult your GP.


