
My partner wanted to help. I could see it in his face — the desperate need to do something useful while I was gripping the side of the bed and making noises neither of us had heard before. But nobody had told him what to actually do. He had not read the birth plan properly. He did not know where anything was in the bag. And when the midwife asked him a question about my preferences, he looked at me — mid-contraction — expecting me to answer.
But when it mattered, he stepped up. I pointed to exactly where the pain was in my lower back and he massaged that spot for about two hours straight. He did not stop, he did not ask questions, he just followed where I guided his hands. That was the most useful thing he did — and it was the one thing nobody had told him to prepare for.
Our baby was born during the Covid period, when restrictions meant fewer people could come in and out of the room. The midwives asked him to help with practical tasks — and he did, without hesitation.
He was not a perfect partner. He was an unprepared one who learned on the job. And that is fixable.
If you are a birth partner reading this, the fact that you are here means you want to do it well. This guide will tell you what actually helps, what does not, and how to be the person she needs when the time comes. And if you are the one having the baby, this is the article to hand to your partner and say: read this.
Quick answer: A birth partner's job is to support, comfort, and advocate. According to the NHS, this means helping with comfort and pain relief, supporting her decisions — even if they change from the birth plan — and communicating with the midwife on her behalf when she cannot do it herself. Research suggests that continuous support during labour is linked with better outcomes, including higher rates of spontaneous vaginal birth.
Before Labour: The Preparation That Actually Matters
Most of what makes a good birth partner happens before the first contraction. The NHS recommends that birth partners prepare by attending antenatal classes, reading the birth plan, and knowing the practical details.
Read the birth plan. Not skim it — actually read it. Know what pain relief she wants to try first. Know what she feels strongly about. Know what the "what if" preferences are. The NCT notes that the midwife caring for her during labour is unlikely to be someone who knows her. You may be the only person in the room who does.
Know where everything is in the hospital bag. You may need to find things while she is busy having a baby. Know where the maternity pads are, where her phone charger is, where the snacks are, and where the baby clothes are.
Know the route to the hospital. Check how long the journey takes at different times of day. The NHS suggests downloading the parking app and having the maternity unit phone number saved in your phone.
Learn the basics of what happens during labour. You do not need a medical degree. But knowing the difference between the latent phase and active labour, understanding what contractions do, and knowing the main pain relief options will stop you from panicking when things get intense.
Practise the comfort techniques. If she is planning to use breathing exercises, practise them together. If she wants back massage or counter-pressure on her hips during contractions, try it beforehand so you know what pressure she likes. But be prepared for it to change during labour — she will guide your hands to the right spot when the time comes, and you may be doing it for a long time. Build your stamina for it.
During Early Labour at Home
Early labour can last hours or even days. This is where your role starts — and it is mostly about keeping things calm.
Time the contractions. Note how long each one lasts and the gap between them. The NHS advises calling the midwife when contractions are regular, lasting at least 60 seconds, and coming every 5 minutes. You can use a phone app or just a clock.
Keep her comfortable. Run a warm bath. Offer a hot water bottle for her back. Make sure she has water and light snacks. Encourage her to rest between contractions if she can.
Be the one who calls the midwife. She may not want to talk on the phone during contractions. Call on her behalf, describe what is happening clearly, and relay the advice back to her.
Do not rush to the hospital too early. The latent phase is often best managed at home. If the maternity unit advises staying at home, trust them — it is not a dismissal, it is because she is more likely to progress well in comfortable surroundings. Your role during this phase is to help her feel safe enough to stay.
If She Is Being Induced
According to the NMPA, around 1 in 3 women and birthing people had an induction of labour in Great Britain in 2023. If this applies to you, the birth partner experience is different from a spontaneous labour — and almost no guide prepares you for it.
Induction is a stepped process. It often begins with a pessary, gel, or balloon catheter to soften the cervix, and this stage alone can take 24 to 48 hours — sometimes longer. Active labour may not start for days. This is normal, but it can feel like an endless wait.
Be prepared for it to be long. Induction is not a quick process. You may spend one, two, or even three days on the antenatal ward waiting for labour to establish. Pack accordingly — your own snacks, a change of clothes, a phone charger, headphones, and something to pass the time. This is a marathon, not a sprint.
Know that you may not be able to stay overnight. Many hospitals do not allow birth partners to stay on the antenatal ward outside of active labour. This means she may be alone overnight during the early stages of induction. Talk about this beforehand so it is not a shock. Make sure she has everything she needs within reach, and agree on how you will stay in touch — a text every hour, a phone call if anything changes.
Manage her expectations and your own. Induction can feel frustrating when nothing seems to be happening. She may feel discouraged, anxious, or bored. Your role during this phase is to keep morale up, stay patient, and remind her that slow progress is still progress.
Stay close when things start moving. Once contractions establish, things can progress quickly after a long wait. Make sure you are contactable at all times and can get to the hospital within a reasonable time. Do not be the partner who missed the birth because they popped home for a nap.
During Labour on the Ward
Once you are at the hospital or birth centre, the pace changes. The midwife is now there, but you are still essential. According to the NCT, women who have continuous support during labour are more likely to have a spontaneous vaginal birth and fewer interventions.
Stay present. Put your phone away unless you are timing contractions or updating family. Be in the room — physically and mentally. The NHS says your role is to comfort her as labour progresses and contractions get stronger.
Offer practical comfort. Hold her hand. Wipe her face with a cool flannel. Offer water through a straw. Rub her back or apply counter-pressure to her hips during contractions if she wants it. According to the NHS, these physical comforts can make a real difference. Do not guess where to massage — ask her to show you. She will know exactly where the pain is. And if she puts your hands on a spot, stay there. I had my partner massaging the same point on my lower back for two hours. It was the single most helpful thing he did.
Be ready to help the staff if asked. During our birth, the Covid restrictions meant fewer people could move in and out of the room, so the midwives asked my partner to help with practical tasks. Even outside of a pandemic, maternity staff may ask you to hold something, pass something, or help reposition a pillow. Do it without hesitation. You are part of the team in that room, not a spectator.
Remind her of her breathing techniques. If she has practised breathing or relaxation exercises, breathe with her if it helps. The NHS suggests this specifically.
Speak to the midwife on her behalf. The NHS says you can help explain to the midwife or doctor what she needs, and help them communicate with her. If something in the birth plan matters to her and it has not been addressed, raise it. You are her voice when she cannot use her own.
Support her decisions — even if they change. She may have written in her birth plan that she did not want an epidural. She may now be asking for one. That is her right. Your job is to support her decisions about pain relief, even if they are different from what is in the birth plan. Do not be the person who says "but you said you didn't want one" while she is in pain. If she is asking, she needs it.
Know what happens if she has an epidural. An epidural is the most effective form of pain relief available during labour. If she decides to have one, an anaesthetist will insert a thin tube into her lower back. She will need to stay very still during the procedure — usually sitting up or lying on her side, curled forward. Your role at this point is to sit in front of her, hold her hands, and help her stay still through contractions while the needle goes in. This can take 10 to 20 minutes. After the epidural is placed, she will have reduced feeling from the waist down, will be attached to a drip and monitor, and her mobility will be limited. She may need help changing position, reaching things, and getting comfortable. The midwife will check on her regularly, but between checks, you become even more important for practical support.
Follow her lead. Her behaviour will change during labour. She may go quiet and not want to talk or be touched. She may say things she does not mean. She may want you close, then need space, then want you close again. Do not take it personally. This is completely normal.
When Plans Change
This is the part of the birth partner role that matters most and gets talked about least.
Labour is unpredictable. The pool might not be available. She might need an assisted delivery. An emergency caesarean might be recommended. In these moments, she may not be in a position to process information and make decisions clearly. That is where you step in.
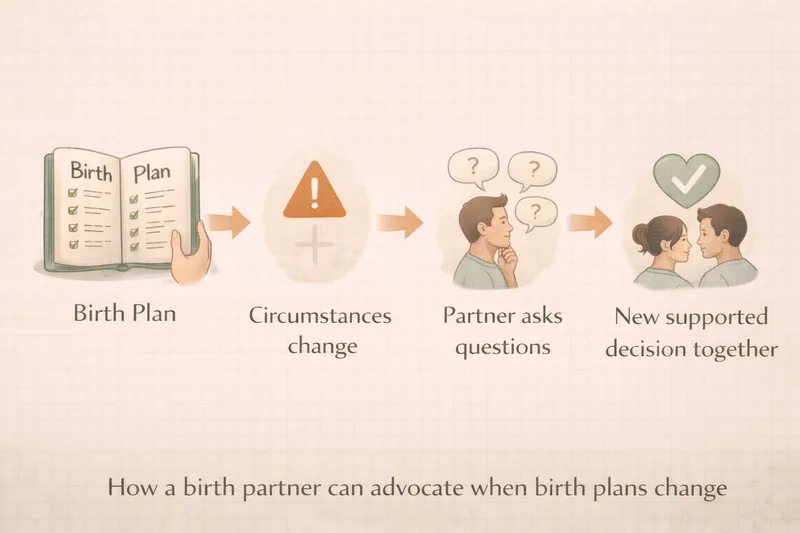
Know the birth plan's "what if" preferences. If she wrote down what she would want in the event of an emergency caesarean, induction, or assisted delivery — you need to know those preferences and be ready to communicate them.
Ask questions. If a member of staff recommends a change of plan, you are allowed to ask why, what the alternatives are, and how urgent it is. A useful question, suggested by NCT's guidance on informed decision-making, is: "Am I in immediate danger? Is my baby in immediate danger?" — this helps establish the actual level of urgency and gives space for a decision rather than a reaction.
Advocate, do not override. Your job is to make sure her voice is heard — not to make decisions for her. If she is conscious and able to communicate, the decision is hers. If she is not able to, you fall back on what she told you she would want.
Stay calm. If things become urgent, the room will fill with professionals who know what they are doing. Your job is not to fix the medical situation — it is to be the steady, familiar presence that helps her feel safe.
After the Birth
Your role does not end when the baby arrives.
Skin-to-skin. If she is unable to hold the baby immediately — for example, after a caesarean or if she is being treated — you can do skin-to-skin contact instead. Place the baby against your bare chest. This helps regulate the baby's temperature and heart rate, and begins the bonding process.
Help with the first feed. If she is planning to breastfeed, she may need practical support — positioning the baby, adjusting pillows, pressing the call button for the midwife if she needs help. You do not need to know how breastfeeding works in detail, but being there and helping with the logistics matters.
Manage visitors and communication. She has just given birth. She is exhausted, emotional, and possibly in pain. You are the gatekeeper. Decide together beforehand who gets told first, who visits and when, and how much contact you both want in the first hours. Then enforce it.
Look after her basic needs. Make sure she has water, food, pain relief if she needs it, and help getting to the bathroom if she is unsteady. On the postnatal ward, she may be alone for long stretches — check that she knows how to call for help and that she has everything within reach before you leave.
Looking After Yourself
Nobody talks about this, but it matters. Labour is intense for birth partners too.
You may feel scared, helpless, overwhelmed, or out of your depth. You may witness things that are difficult to process. You may feel guilty that you cannot take the pain away. All of this is normal.
Eat and drink. You cannot support someone else if you are running on empty. Pack your own snacks and keep yourself hydrated.
Take a break if you need one. A five-minute walk to get some air or a cup of tea is not abandoning her — it is making sure you can keep going.
Talk about it afterwards. Birth can be emotionally intense for partners. If you are struggling with what you saw or experienced, speak to your GP or a mental health professional. Your feelings are valid and you are allowed to process them.
Frequently Asked Questions
What if I feel faint or cannot cope during the birth? This is more common than you think. Tell the midwife. Sit down, have some water, and take a moment. It is better to step out briefly than to faint and become a patient yourself.
Can I cut the umbilical cord? According to the NHS, your birth partner may be able to cut the umbilical cord. Talk to the midwife about this in advance. It is not compulsory — only do it if you want to.
What if I do not know what to do? Ask the midwife. They deal with nervous birth partners every day. They will tell you where to stand, what to do, and how to help. You do not need to know everything — you just need to be there and be willing to follow her lead.
Can two people be birth partners? Many hospitals allow up to two birth partners during established labour, but policies vary by maternity unit. Check with your unit in advance.
What should I do during an induction? Induction can take days. Bring your own supplies — snacks, a charger, comfortable clothes, entertainment. You may not be allowed to stay overnight on the antenatal ward, so agree a communication plan with her in advance. When active labour starts, things can move quickly — stay contactable and ready to come in.
What if she says something hurtful during labour? She does not mean it. Labour is one of the most physically intense experiences a person can go through. If she tells you to stop touching her or shouts at you, it is the pain talking. Do not take it personally, and do not hold it against her afterwards.
What should I do if she asks for an epidural she didn't want? Support her. Birth plans are preferences, not contracts. If she is asking for an epidural, she has decided she needs it — and that decision is hers to make. Do not question it, do not remind her of the plan, and do not make her feel guilty. When the anaesthetist arrives, your job is to help her stay still during the procedure by sitting in front of her and holding her hands through contractions. After the epidural is in, she will need more practical help — changing position, reaching water, staying comfortable — because her mobility will be reduced.
The Bottom Line
Being a birth partner is not about having all the answers. It is about being present, prepared, and willing to put her needs first. Read the birth plan. Know where things are. Learn a few practical comfort techniques. And when things get intense, be the calm, steady person who makes sure her voice is heard.
The best birth partners are not the ones who know the most about labour. They are the ones who listened, prepared, and showed up ready to do whatever was needed — even if that meant standing quietly in the corner holding her hand while the professionals did their work.
You cannot take the pain away. But you can make sure she is not alone in it.
This article is for general information only and does not replace advice from your midwife or maternity team. Every labour is different — this guide covers practical ways a birth partner can help, based on NHS guidance and real experience.
This article was written in April 2026. We regularly review our content against the latest NHS and NICE guidelines to help ensure accuracy. This article references NHS: Tips for Your Birth Partner, NHS Start for Life: Tips for Your Birthing Partner, NCT: Birth Partners and Doulas, NCT: Maternity Rights and Informed Decision Making, and RCOG/NMPA: State of the Nation Report 2023. If you have questions about the birth partner role, speak to your midwife.


